Instructions
Method of administration and dosage
Orally, during meals.
Prevention of lactation: 1 mg once (2 tablets of 0.5 mg), on the first day after childbirth (preferably with the first meal after childbirth).
Suppression of established lactation: 0.25 mg (1/2 tablet) 2 times a day every 12 hours for two days (the total dose is 1 mg). In order to reduce the risk of orthostatic arterial hypotension in a woman, a single dose of cabergoline should not exceed 0.25 mg.
Treatment of hyperprolactinemia-related disorders: The recommended starting dose is 0.5 mg per week, administered once (1 tablet of 0.5 mg) or in two divided doses (1/2 tablet of 0.5 mg, for example, on Monday and Thursday). The weekly dose should be gradually increased by 0.5 mg at monthly intervals until the optimal therapeutic effect is achieved. The therapeutic dose is usually 1 mg per week, but can range from 0.25 to 2 mg per week. The maximum dose for patients with hyperprolactinemia should not exceed 4.5 mg per week.
Depending on tolerability, the weekly dose can be taken once or divided into 2 or more doses per week. Dividing the weekly dose into several doses is recommended when prescribing the drug at a dose of more than 1 mg per week.

In patients with increased sensitivity to dopaminergic drugs, the likelihood of adverse reactions can be reduced by starting cabergoline therapy at a lower dose (e.g., 0.25 mg once a week), followed by a gradual increase until the therapeutic dose is reached. To improve tolerability of the drug, if severe adverse reactions occur, a temporary dose reduction is possible, followed by a more gradual increase (e.g., an increase of 0.25 mg per week or every 2 weeks).
When increasing the dose, patients should undergo regular examination to establish the lowest effective dose of cabergoline. It is recommended to determine the concentration of prolactin in the blood plasma at least once a month, since normalization of its concentration usually occurs within 2-4 weeks after selecting an effective dose of Dostinex.
After discontinuation of Dostinex®, a relapse of hyperprolactinemia is usually observed. However, some patients experience a persistent decrease in the concentration of prolactin in the blood plasma for several months. Most women continue to have ovulatory cycles for at least 6 months after stopping therapy.
- Use of the drug in special clinical patient groups
- In children and adolescents
- The efficacy and safety of Dostinex in children and adolescents aged 16 years have not been established.
- In elderly patients
- Due to the indications for use of cabergoline, experience with its use in elderly patients is extremely limited. Available data do not indicate any special risk.
- In patients with liver dysfunction
- In patients with severe liver failure, lower doses of Dostinex should be used.
Indications
- Prevention of physiological lactation after childbirth.
- Suppression of established postpartum lactation.
- Treatment of disorders associated with hyperprolactinemia, including amenorrhea, oligomenorrhea, anovulation, galactorrhea.
- Prolactin-secreting pituitary adenomas (micro- and macroprolactinomas); idiopathic hyperprolactinemia; empty sella syndrome in combination with hyperprolactinemia.
Composition
Each tablet contains:
- Active ingredient: cabergoline 0.50 mg;
- Excipients: lactose 75.90 mg, leucine 3.60 mg.
Contraindications
- Hypersensitivity to cabergoline and/or any excipient in the drug, as well as to any ergot alkaloids.
- History of fibrotic changes in the lungs, pericardium or retroperitoneum.
With long-term therapy: anatomical signs of heart valve pathology (such as valve leaflet thickening, valve lumen narrowing, mixed pathology of valve narrowing and stenosis), confirmed by echocardiography (EchoCG) performed before the start of therapy.
- Use in children and adolescents under 16 years of age (the safety and efficacy of the drug have not been established).
- Lactose intolerance, lactase deficiency, glucose-galactose malabsorption.
- Pregnancy and breastfeeding (due to the lack of clinical data on the efficacy and safety of cabergoline).
With caution
Like other ergot derivatives, cabergoline should be prescribed with caution in the following conditions or diseases:
- arterial hypertension that developed during pregnancy, such as preeclampsia or postpartum arterial hypertension (Dostinex is prescribed only in cases where the potential benefit from the use of the drug significantly outweighs the possible risk);
- severe cardiovascular diseases, Raynaud's syndrome;
- peptic ulcer, gastrointestinal bleeding;
- severe liver failure (lower doses are recommended);
- severe psychotic or cognitive impairment (including history);
- concomitant use with drugs that have an antihypertensive effect (due to the risk of orthostatic arterial hypotension);
Special instructions
Before initiating cabergoline therapy for hyperprolactinemia-related disorders, a complete pituitary examination should be performed.
Before initiating long-term cabergoline therapy, all patients should undergo a cardiovascular examination, including an echocardiogram (to exclude asymptomatic heart defects). In addition, determination of CRP or other inflammatory markers, chest radiography, pulmonary function testing, and renal function testing are advisable.
As with other ergot derivatives, pleural effusion/pleural fibrosis and valvulopathy have been reported in patients treated with cabergoline for a long time. In some cases, patients have received prior therapy with ergotamine dopamine agonists. Therefore, cabergoline should not be used in patients with signs and/or clinical symptoms of cardiac or respiratory dysfunction associated with fibrotic changes or with a history of such conditions. The drug should be discontinued if signs of new or worsening regurgitation, valvular narrowing or thickening of the valve leaflets are detected.

The erythrocyte sedimentation rate has been shown to increase with the development of pleural effusion or fibrosis. In case of unexplained increase in the erythrocyte sedimentation rate, chest radiography is recommended. Determination of plasma creatinine and assessment of renal function may be helpful in establishing the diagnosis. Improvement of symptoms was observed in patients with pleural effusion/pleural fibrosis or valvulopathy after discontinuation of cabergoline.
It is unknown whether cabergoline can worsen the condition of patients with signs of blood regurgitation. Dostinex should not be used if fibrotic lesions of the valvular heart apparatus are detected.
Fibrotic disorders can develop asymptomatically. Therefore, patients receiving long-term cabergoline therapy should be regularly monitored and special attention should be paid to the following symptoms:
- pleuro-pulmonary disorders: such as dyspnea, difficulty breathing, persistent cough or chest pain;
- renal failure or obstruction of the ureters or abdominal organs, which may be accompanied by pain in the side or in the lumbar region and swelling of the lower extremities, any swelling or tenderness to touch in the abdomen, which may indicate the development of retroperitoneal fibrosis;
- pericardial fibrosis and fibrosis of the heart valve leaflets often manifest as heart failure. In this regard, it is necessary to exclude fibrosis of the heart valve leaflets (and constrictive pericarditis) when symptoms of heart failure appear.
The patient's condition should be regularly monitored for the development of fibrotic disorders. The first echocardiogram should be performed 3-6 months after the start of therapy. Then this study should be repeated depending on the clinical assessment of the patient's condition, paying particular attention to the symptoms described above, at least every 6-12 months of therapy.
The need for other monitoring methods (e.g. physical examination, including cardiac auscultation, radiography, computed tomography) is assessed individually for each patient.
Cabergoline restores ovulation and fertility in women with hyperprolactinemic hypogonadism. Pregnancy should be excluded before starting cabergoline. Since pregnancy may occur before menstruation is restored, pregnancy tests are recommended at least once every 4 weeks during the period of amenorrhea, and after the restoration of menstruation - every time a delay in menstruation is noted for more than 3 days. Women wishing to avoid pregnancy should use barrier methods of contraception during treatment with cabergoline, as well as after discontinuation of the drug until anovulation reoccurs. Women who become pregnant should be monitored by a physician for timely detection of symptoms of pituitary enlargement, since pre-existing pituitary tumors may increase in size during pregnancy.
In patients with severe hepatic impairment, low doses of cabergoline should be used for long-term therapy. In patients with severe hepatic impairment (Child-Pugh class C), after a single dose of 1 mg cabergoline, the AUC value was higher than in healthy volunteers or patients with less severe hepatic impairment.
Cabergoline causes drowsiness. In patients with Parkinson's disease, dopamine agonists may cause sudden sleep onset. In such cases, it is recommended to reduce the cabergoline dose or discontinue therapy.
Cabergoline is not recommended for use in patients with renal impairment, due to the lack of clinical data on the efficacy and safety of cabergoline in this patient population.
Patients should be regularly monitored for signs of impulse control disorders during long-term cabergoline therapy, and patients and/or caregivers should be informed about the possible development of behavioral disorders during therapy. Impulse control disorders such as pathological gambling, increased libido, and hypersexuality have been reported in patients receiving dopaminergic receptor agonists, including cabergoline. These events were usually reversible upon dose reduction or discontinuation of the drug.
Packaging and release form
0.5 mg tablets - 2 pieces with instructions for use in the package.
Side effects
During clinical studies using cabergoline to prevent physiological lactation (1 mg once) and to suppress lactation (0.25 mg every 12 hours for 2 days), adverse reactions were observed in approximately 14% of women. When using cabergoline for 6 months at a dose of 1-2 mg per week, divided into 2 doses, to treat disorders associated with hyperprolactinemia, the frequency of adverse reactions was 68%. Adverse reactions occurred mainly during the first 2 weeks of therapy and in most cases disappeared as therapy continued or a few days after discontinuing cabergoline. Adverse reactions were usually transient, mild to moderate in severity and dose-dependent. At least once during therapy, severe adverse reactions were observed in 14% of patients; due to adverse reactions, treatment was discontinued in approximately 3% of patients.
Possible adverse reactions when using cabergoline are distributed by system-organ classes with an indication of their frequency of occurrence according to WHO recommendations (very common (1/10); common (1/100 to <1/10); uncommon (1/1,000 to <1/100); rare (1/10,000 to <1/1,000); very rare (<1/10,000), unknown (cannot be determined on the basis of available data):
System organ class Very common, Common, Uncommon, Rare, Very rare, Frequency unknown
Immune system disorders hypersensitivity reactions
Psychiatric disorders depression increased libido aggressiveness, delusions, hypersexuality, gambling addiction/pathological gambling, psychotic disorders, hallucinations
Nervous system disorders headache, dizziness/vertigo drowsiness transient hemianopsia, syncope (short-term fainting with loss of consciousness), paresthesia attacks of sudden sleep onset, tremor
Visual disorders visual impairment
Cardiac disorders valvular heart disease (valvulopathy), including regurgitation, and associated disorders (pericarditis and pericardial effusion) palpitations angina pectoris
Vascular disorders with long-term use cabergoline usually has an antihypertensive effect action, in some cases orthostatic arterial hypotension, "hot flashes" spasm of blood vessels of the upper and lower extremities, fainting may occur
Disorders of the respiratory system, thoracic organs and mediastinum dyspnea, pleural effusion, fibrosis (pulmonary fibrosis), nosebleed pleural fibrosis respiratory failure, respiratory failure, pleurisy and chest pain
Disorders of the gastrointestinal tract nausea, dyspepsia, gastritis, abdominal pain constipation, vomiting pain in the epigastric region
Disorders of the liver and biliary tract liver dysfunction
Disorders of the skin and subcutaneous tissues rash, alopecia
Disorders of the musculoskeletal and connective tissue lower extremity cramps
Disorders of the genitals and mammary glands mastodynia
General disorders and disorders at the injection site asthenia, increased fatigue edema, peripheral edema
Laboratory and instrumental data asymptomatic decrease in blood pressure (systolic - not less than 20 mm Hg; diastolic - not less than 10 mm Hg) possible decrease in hemoglobin content in women with amenorrhea in the first months after the resumption of menstruation deviation from the norm of standard laboratory parameters during long-term therapy with cabergoline increased creatine phosphokinase activity, abnormal liver function tests
Impulse control disorders: pathological addiction to gambling, increased libido, hypersexuality, a tendency to inappropriate spending or compulsive buying, bulimic overeating and bulimia may occur in patients receiving therapy with dopaminergic receptor agonists, including cabergoline.
Pharmacotherapeutic group
dopamine receptor agonist
Interaction with other medicinal products
There is no information on the interaction of cabergoline and other ergot alkaloids, therefore, the simultaneous use of these drugs during long-term therapy with Dostinex is not recommended.
Since cabergoline exerts a therapeutic effect by direct stimulation of dopamine receptors, it cannot be prescribed simultaneously with drugs that act as dopamine antagonists (phenothiazines, butyrophenones, thioxanthenes, metoclopramide, domperidone, alizapride, etc.), since they can weaken the effect of cabergoline aimed at reducing prolactin concentrations.
Like other ergot derivatives, Dostinex cannot be used simultaneously with macrolide antibiotics (eg, erythromycin, josamycin, troleandomycin), since this may lead to an increase in the systemic bioavailability of cabergoline.
Effect on ability to drive a car and other mechanisms
Patients taking cabergoline should refrain from driving vehicles and mechanisms and other potentially dangerous activities that require concentration and speed of psychomotor reactions.
How to order?
Dostinex (cabergoline) - You can buy in a Canadian online pharmacy. To see our offer, follow the link above. High quality generic and favorable cost of Dostinex (generic) guaranteed. Buying Dostinex over the counter (otc) is an economical solution without risk. When ordering the drug, you do not need a prescription, you do not need one to buy generics. We sell only high-quality drugs and deliver by mail - anonymously. See our offer and buy profitably. We offer the best price and fast delivery! For repeat orders, you have a discount of up to 20%.
Use during pregnancy and breastfeeding
Pregnancy
There are no adequate, controlled clinical studies on the use of cabergoline in pregnant women. Animal studies have not demonstrated a teratogenic effect of cabergoline, but decreased fertility and embryotoxicity were found. Results of a 12-year observational study of the effect of cabergoline on pregnancy outcomes showed that 6.6% (17 out of 256 pregnancies) resulted in serious congenital malformations or premature termination of pregnancy (the most common were malformations of the musculoskeletal system, heart and lungs). There is no information on perinatal disorders or long-term observations of the development of newborns whose mothers took cabergoline during pregnancy. In this regard, cabergoline therapy during pregnancy is possible only in cases of extreme necessity, taking into account a careful assessment of the benefit-risk ratio for the woman and the fetus. Given the long half-life of cabergoline and the limited data on the effect of cabergoline on the fetus, patients planning pregnancy should stop taking it one month before the planned date of pregnancy. If pregnancy occurs during cabergoline therapy, the drug should be discontinued after pregnancy is confirmed.
Breastfeeding period
Cabergoline penetrates into the milk of lactating rats; there is no information on the penetration of cabergoline into human breast milk. However, if there is no sufficient effect of cabergoline to prevent or suppress lactation, breastfeeding should be discontinued.
Since cabergoline prevents lactation, the drug is contraindicated for patients with hyperprolactinemia planning to breastfeed.
Pharmacodynamics
Cabergoline is a dopaminergic derivative of ergoline and is characterized by a pronounced and prolonged prolactin-lowering effect due to direct stimulation of D2-dopamine receptors of pituitary lactotropic cells. In addition, when taking higher doses compared to those for reducing prolactin concentration in blood plasma, cabergoline has a central dopaminergic effect due to stimulation of D2 receptors.
A decrease in the concentration of prolactin in the blood plasma is observed within 3 hours after taking the drug and lasts for 7-28 days in healthy volunteers and patients with hyperprolactinemia, and up to 14-21 days in women in the postpartum period.
Cabergoline has a strictly selective effect, does not affect the basal secretion of other pituitary hormones and cortisol. The prolactin-lowering effect of cabergoline is dose-dependent both in terms of severity and duration of action.
The pharmacodynamic effects of cabergoline that are not associated with the therapeutic effect include only a decrease in blood pressure (BP). With a single dose of the drug, the maximum hypotensive effect is observed within the first 6 hours and is dose-dependent.
Pharmacokinetics
Absorption
Cabergoline is rapidly absorbed from the gastrointestinal tract, the maximum concentration in the blood plasma after a single oral dose of 0.5 mg to 1.5 mg is 30-70 pg / ml and is achieved in 2-3 hours. The absolute bioavailability of cabergoline is unknown. Food intake does not affect the absorption and distribution of cabergoline.
Distribution
Binding to plasma proteins is 41-42%.
Metabolism
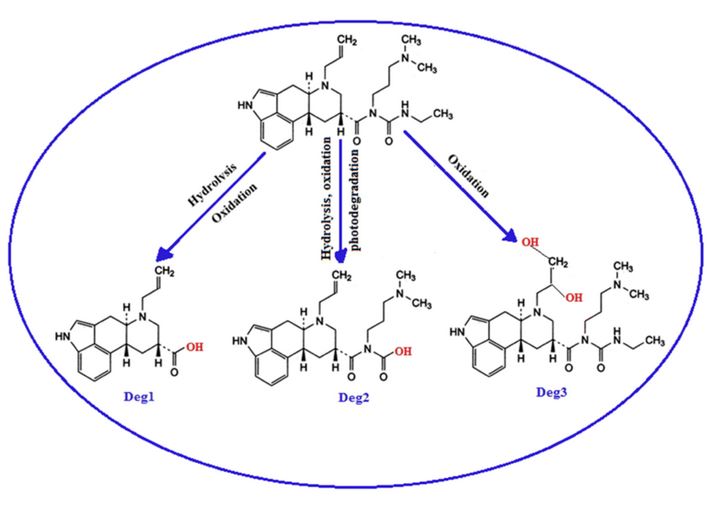
The main metabolite of cabergoline identified in urine is 6-allyl-8β-carboxy-ergoline at a concentration of up to 4-6% of the dose taken, the concentration of 3 additional metabolites is less than 3% of the dose. Metabolites have a significantly lesser effect on suppression of prolactin secretion compared to cabergoline.
Elimination
The half-life of cabergoline, estimated from the rate of renal elimination, is 63-68 hours in healthy volunteers and 79-115 hours in patients with hyperprolactinemia. Due to the long half-life, steady-state concentrations of cabergoline are reached after 4 weeks. Ten days after taking cabergoline, approximately 18% and 72% of the dose taken are found in urine and feces, respectively, with the proportion of unchanged cabergoline in urine being 2-3%.
Overdose
Symptoms of overdose (most likely symptoms of dopamine receptor hyperstimulation): nausea, vomiting, dyspeptic disorders, orthostatic arterial hypotension, confusion, psychosis, hallucinations.
In case of overdose, supportive measures should be taken to remove the unabsorbed drug (gastric lavage) and, if necessary, maintain blood pressure. Dopamine antagonists may be prescribed.